




Let’s look at how to use CPT as a medical coder.
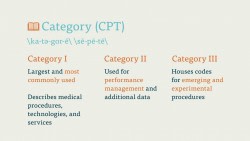
Remember, the CPT code is divided into three categories. Most coders spend the majority of their time with Category I, which describes procedures, services, and technologies administered by healthcare professionals.
Category I is divided into six sections, which are grouped, for the most part, in numerical order. The sections are Evaluation and Management (E&M), Anesthesia, Surgery, Radiology, Pathology and Laboratory, and Medicine. These sections, with the exception of E&M, are in loose numerical order, though you may find some codes from one section referenced in another section.
When you’re coding, you first want to think about what kind of procedure you’re looking at. Was it a patient visit? A surgical procedure? Did a physician administer an X-ray? Did they prescribe medication to the patient? Using that information, you can start looking at higher and higher levels of specificity. Where on the patient’s body was the surgery performed? Where was the X-ray?
As a coder, your job is to use this information to find the best possible code for the procedure.
As with ICD codes, the process of procedure coding begins with a physician’s report. The coder reads this report, makes notes of the important procedures and terms used in the report, and then uses this information to determine the best CPT code to input. Let’s take a look at a quick, simple example.
A patient breaks his arm and must go to the emergency room. His injury is serious, but is not a risk to the patient’s life or major physiological functions. Leaving aside the other procedures that a physician would undoubtedly perform in this situation, let’s look only at the hospital visit itself as a procedure code.
Since this is an instance of Evaluation and Management (E&M), we would turn to the first section of the CPT book. We’d find the “Emergency Department Services” subsection and look at the codes listed there. There are a number of codes for a trip to the ER, and so we have to pick the one that fits our situation best. We’d select 99282 for an “Emergency department visit” of “low to moderate severity.” There are higher and lower levels of severity, but this code fits the visit best: the patient has a moderately severe injury but is in no serious danger.
Like ICD codes, when coding with CPT we always want to code to the highest level of specificity. We never want to stop coding at a CPT code that is simply “close enough” to the procedure performed. In E&M situations, this may be a bit of a judgment call, but as the procedures get more and more specific, there is less room for interpretation.
Here’s a slightly more complicated example. A patient requires the biopsy of a deep, intramuscular cyst in his elbow. This is a surgical procedure, so we’d find the code in the surgery section of the CPT codebook. This is also a procedure related to the musculoskeletal system, which is the first subsection of the Surgery section, so we’d flip toward the front of the section. We’d locate the correct part of the body that the surgery is performed on, the humerus (upper arm) and elbow.
From there we’d look at excision codes. The first one that comes up is the excision of soft tissue of the upper arm.
Parent Codes
Now is a good time to recall something that we learned earlier. There are indented, or parent codes, in the CPT book. Certain procedures, like the excision of soft tissue for a biopsy in the upper arm, have important variations. In our example, there are two options for this procedure: an excision of soft tissue on the skin of the upper arm, and an excision of soft tissue deep in the arm. The latter procedure is indented below the former. The former is the parent code. The specification of the parent code comes after a semi-colon, and describes where the excision takes place.
When using the indented code, we’d replace what comes after the semicolon with the procedure listed in the indented code.
Here’s the parent code: 24065 – Biopsy, soft tissue of upper arm or elbow area; superficial.
And here’s the code we want: 24066 – Biopsy, soft tissue of upper arm or elbow area; deep (subfascial or intramuscular).
So we’d select the indented code (24066) and use that as the procedure code for the biopsy on the cyst in our patient’s elbow.
In certain cases, you may find that the procedure you’ve been asked to code cannot be found in the CPT code manual. Remember that we want to code as accurate as possible at all times. In cases where a procedure has not yet made it’s way into the CPT book, we use an unlisted procedure code and file an additional report.
Out of order codes
Sometimes you may find procedure codes that are out of order in the code manual. Placing codes out of numerical order allows for clustering of similar procedures, and can help the medical coder find exactly the right procedure code. These out-of-sequence codes typically have a note instructing the coder to flip to the correct code elsewhere in the book. Think of these out-of-sequence codes as road signs.
Guidelines
The CPT codebook is full of guidelines. Each section of Category I has guidelines specific to that section. The Anesthesia section, for example, instructs coders on how to code the duration of the anesthetic procedure.
Many codes also have guidelines or instructions, and this is where the CPT code set can get very complex. Certain procedures, like a “photodynamic therapy of second eye” (code 67225), must be used in conjunction with another procedure. In this case, code 67225 must be coded along with code 67221, for “photodynamic therapy (includes intravenous infusion).”
Other codes may instruct you not to report this code in conjunction with a certain other code. Those procedures may contradict one another or overlap.
Some codes will also have instructions, listed in parentheses, that instruct the coder to look elsewhere for a procedure. Let’s say a coder receives a medical report that a patient had the ACL in his knee reconstructed during a surgical procedure. That coder would turn to the Surgery section of the code book, then to the musculoskeletal subsection. The coder would find the section on the femur and knee joint, and look at code 27407 – “repair, primary, torn ligament and/or capsule, knee; cruciate.”
The coder would then look at the instructions below this code and see a note: “For cruciate ligament reconstruction, use 27427.” The medical coder needs to describe a reconstruction, not a repair, and so the first code—27407—would be incorrect. The coder would go to 27427, check that it is the correct procedure, and then use that code.
These guidelines and instructions may seem redundant, highly specific, or needlessly complicated, but insurance companies need as much information as possible in order to properly gauge the authority of a medical claim. When in doubt, always follow the rules laid out by the CPT code set.
Code Symbols
In an effort to save space, and save you from having to read tedious notes on each and every code, the CPT Editorial Board has instituted a number of symbols within the codebook. These symbols will tell you important information about the code. Each codebook will have a key that explains these symbols.
We won’t dive fully into all of these symbols, but you should know about a few of the more common ones.
Part of the purpose of the code symbols included in the CPT manual is to tell coders which codes are new, resequenced, or revised procedure codes. The new procedures are marked with a red dot. Heavily revised procedures are marked with a blue triangle. New and revised procedure descriptions are marked with green triangles.
These code symbols also illustrate which codes must be, or cannot be, used in conjunctions with other codes. Certain codes are always paired with other codes. These are called “add-on” codes, and are noted with a boldfaced plus sign. Other codes are incompatible with the -51 modifier, and are marked with a circle with a diagonal line through it. We’ll cover what a -51 modifier is in the next section—or now, just know that a procedure marked like this cannot be part of a “multiple procedure” report.
Appendices
When you’re using a code set as large and complicated as CPT, it helps to have a place to turn to for information specific to certain parts of the code set. The appendices at the back of the CPT manual allow you to search newly added codes, CPT modifiers, and a list of CPT add-on codes.
Index
Finally, we come to the index. The CPT Index can be used like any other index. You can use it to track down hard-to-code procedures, services, and tests, and you can search it by both procedure and body part.
However, a trained medical coder never codes from the index. It is merely a tool for finding the right information.
Let’s close this course with a quick example of a coder using the index the right way.
A patient receives an X-ray of both their femoral arteries. The medical report is passed to the coder. The coder knows this is a radiology code, but isn’t sure which procedure to code. She turns to the index and finds Artery, Femoral, but can’t find the proper procedure. The coder is looking for the code for a venography, which is an invasive procedure that uses a catheter filled with dye, which is injected and traced through the body via X-ray.
The coder turns instead to Venography in the index and finds the code range for venographies in the leg: 75820-75822. The coder turns to this section and finds a number of venographies, each for a specific part of the body. The coder chooses the first one, 75822, for a bilateral venography of the extremities, with radiological supervision and interpretation.
Moving Forward
In the next course, we’ll learn how CPT modifiers can help us code more accurately, and with a wider range of information.
